
Cleft lip and cleft palate are facial and oral malformations that occur very early in pregnancy, while the baby is developing inside the mother. Clefting results when there is not enough tissue in the mouth or lip area, and the tissue that is available does not join together properly.
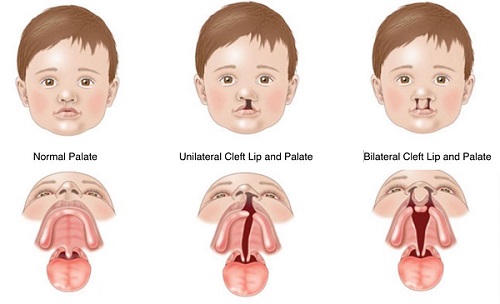
A cleft lip is a physical split or separation of the two sides of the upper lip and appears as a narrow opening or gap in the skin of the upper lip. This separation often extends beyond the base of the nose and includes the bones of the upper jaw and/or upper gum.
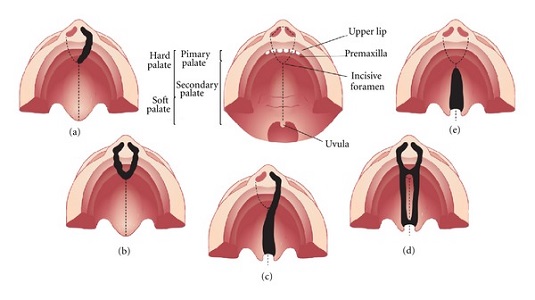
A cleft palate is a split or opening in the roof of the mouth. A cleft palate can involve the hard palate (the bony front portion of the roof of the mouth), and/or the soft palate (the soft back portion of the roof of the mouth).
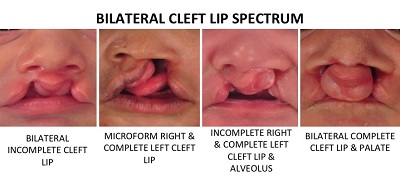
Cleft lip and cleft palate can occur on one or both sides of the mouth. Because the lip and the palate develop separately, it is possible to have a cleft lip without a cleft palate, a cleft palate without a cleft lip, or both together.
Who Gets Cleft Lip and Cleft Palate?
Cleft lip, with or without cleft palate, affects one in 700 babies annually, and is the fourth most common birth defect in the India. Clefts occur more often in children of Asian, Latino, or Native American descent. Compared with girls, twice as many boys have a cleft lip, both with and without a cleft palate. However, compared with boys, twice as many girls have cleft palate without a cleft lip.
What Causes a Cleft Lip and Cleft Palate?
In most cases, the cause of cleft lip and cleft palate is unknown. These conditions cannot be prevented. Most scientists believe clefts are due to a combination of genetic and environmental factors. There appears to be a greater chance of clefting in a new-born if a sibling, parent, or relative has had the problem.
Another potential cause may be related to a medication a mother may have taken during her pregnancy. Some drugs may cause cleft lip and cleft palate. Among them: anti-seizure/anticonvulsant drugs, acne drugs containing Accutane, and methotrexate, a drug commonly used for treating cancer, arthritis, and psoriasis.
Cleft lip and cleft palate may also occur as a result of exposure to viruses or chemicals while the foetus is developing in the womb. In other situations, cleft lip and cleft palate may be part of another medical condition.
How Are Cleft Lip and Cleft Palate Diagnosed?
Because clefting causes very obvious physical changes, a cleft lip or cleft palate is easy to diagnose. Prenatal ultrasound can sometimes determine if a cleft exists in an unborn child. If the clefting has not been detected in an ultrasound prior to the baby's birth, a physical exam of the mouth, nose, and palate confirms the presence of cleft lip or cleft palate after a child's birth. Sometimes diagnostic testing at best hospitals for cleft palate surgery in Mysore may be conducted to determine or rule out the presence of other abnormalities.
What Problems Are Associated With Cleft Lip and/or Palate?
Eating problems. With a separation or opening in the palate, food and liquids can pass from the mouth back through the nose. Fortunately, specially designed baby bottles and nipples that help keep fluids flowing downward toward the stomach are available. Children with a cleft palate may need to wear a man-made palate to help them eat properly and ensure that they are receiving adequate nutrition until surgical treatment is provided.
Ear infections/hearing loss. Children with cleft palate are at increased risk of ear infections since they are more prone to fluid build-up in the middle ear. If left untreated, ear infections can cause hearing loss. To prevent this from happening, children with cleft palate usually need special tubes placed in the eardrums to aid fluid drainage, and their hearing needs to be checked once a year.
Speech problems. Children with cleft lip or cleft palate may also have trouble speaking. These children's voices don't carry well, the voice may take on a nasal sound, and the speech may be difficult to understand. Not all children have these problems and surgery may fix these problems entirely for some. For others, a special doctor, called speech pathologist, will work with the child to resolve speech difficulties.
Dental Problems. Children with clefts are more prone to a larger than average number of cavities and often have missing, extra, malformed, or displaced teeth requiring dental and orthodontic treatments. In addition, children with cleft palate often have an alveolar ridge defect. The alveolus is the bony upper gum that contains teeth. A defect in the alveolus can (1) displace, tip, or rotate permanent teeth, (2) prevent permanent teeth from appearing, and (3) prevent the alveolar ridge from forming. These problems can usually be repaired through oral surgery. at dental hospitals in Mysuru.
Who Treats Children With Cleft Lip and/or Palate?
Due to the number of oral health and medical problems associated with a cleft lip or cleft palate, a team of doctors and other cleft lip surgery specialists in Mysore is usually involved in the care of these children. Members of a cleft lip and palate team typically include:
- Cleft Surgeon – Plastic Surgeon/ Maxillofacial Surgeon to evaluate and perform necessary surgeries on the lip and/or palate.
- An otolaryngologist (an ear, nose, and throat doctor) to evaluate hearing problems and consider treatment options for hearing problems.
- An oral surgeon to reposition segments of the upper jaw when needed, to improve function and appearance and to repair the cleft of the gum.
- An orthodontist to straighten and reposition teeth.
- A dentist to perform routine dental care.
- A prosthodontist to make artificial teeth and dental appliances to improve the appearance and to meet functional requirements for eating and speaking.
- A speech pathologist to assess speech and feeding problems.
- A speech therapist to work with the child to improve speech.
- An audiologist (a specialist in communication disorders stemming from a hearing impairment); to assess and monitor hearing.
- A nurse coordinator to provide ongoing supervision of the child's health.
- A social worker/psychologist to support the family and assess any adjustment problems.
- A geneticist to help parents and adult patients understand the chances of having more children with these conditions.
The health care team works together to develop a plan of care to meet the individual needs of each patient. Treatment usually begins in infancy and often continues through early adulthood.
What’s the Treatment for Cleft Lip and Cleft Palate?
A cleft lip may require one or two surgeries depending on the extent of the repair needed. The initial Cleft lip surgery in Mysuru is usually performed by the time a baby is 3 months old.
Repair of a cleft palate often requires multiple surgeries over the course of 18 years. The first surgery to repair the palate usually occurs when the baby is between 6 and 12 months old. The initial cleft palate surgery in Mysore creates a functional palate, reduces the chances that fluid will develop in the middle ears, and aids in the proper development of the teeth and facial bones.
Children with a cleft palate may also need a bone graft when they are about 8 years old to fill in the upper gum line so that it can support permanent teeth and stabilize the upper jaw. About 20% of children with a cleft palate require further surgeries to help improve their speech.
Once the permanent teeth grow in, braces are often needed to straighten the teeth.
Additional surgeries may be performed by best doctors of cleft lip surgery in Mysuru to improve the appearance of the lip and nose, close openings between the mouth and nose, help breathing, and stabilize and realign the jaw. Final repairs of the scars left by the initial surgery will probably not be performed until adolescence, when the facial structure is more fully developed.
What Is the Outlook for Children With Cleft Lip and/or Cleft Palate?
Although treatment for a cleft lip and/or cleft palate may extend over several years and require several surgeries depending upon the involvement, most children affected by this condition can achieve normal appearance, speech, and eating.
Dental Care for Children with Cleft Lip and/or Palate
Generally, the preventive and restorative dental care needs of children with clefts are the same as for other children. However, children with cleft lip and cleft palate may have special problems related to missing, malformed, or malpositioned teeth that require close monitoring.
Early dental care. Like other children, children born with cleft lip and cleft palate require proper cleaning, good nutrition, and fluoride treatment in order to have healthy teeth. Appropriate cleaning with a small, soft-bristled toothbrush should begin as soon as teeth erupt. Many dentists recommend that the first dental visit be scheduled at about 1 year of age or even earlier if there are special dental problems. Routine dental care can begin around 1 year of age.
Orthodontic care. A first orthodontic appointment may be scheduled before the child has any teeth. The purpose of this appointment is to assess facial growth, especially jaw development. After teeth erupt, an orthodontist can further assess a child's short and long-term dental needs. After the permanent teeth erupt, orthodontic treatment can be applied to align the teeth.
Prosthodontic care. A prosthodontist is a member of the cleft palate team. He or she may make a dental bridge to replace missing teeth or make special appliances called "speech bulbs" or "palatal lifts" to help close the nose from the mouth so that speech sounds more normal. The Prosthodontist coordinates treatment with the Oral & Maxillofacial Surgeon or Plastic Surgeon and with the speech pathologist.
Surgical Repair of Cleft Lip and Palate Treatment Protocol – Precision Centre Dr Ravi Kumar M P
Surgical procedures required for each patient with cleft lip and palate will vary depending upon the type and severity of the deformity. Timing and treatment will be adjusted based on each patient’s overall medical needs, but treatment typically includes a combination of the procedures explained here, performed within general time frames based on development.
Read on below for an introduction to the various procedures that may be included in the surgical repair of cleft lip and cleft palate. Surgery for both cleft lip and cleft palate require general anaesthesia in the hospital based setup which covers comprehensive care for the paediatric patients. We have a set of TEAM Member – Surgeons, Paediatrician, Anaesthesiologist, Nursing Staff and others who have been associated in management of this care since 2009 in Mysuru.
For more details about your child’s specific procedure and follow-up care, please consult your surgeon, Dr. Ravi Kumar MP or other members of our team. We are available any time to answer all of your treatment questions.
Naso Alveolar Molding
1 week to 3 months of age (if needed)
Babies born with unilateral cleft lip or unilateral cleft lip and palate have the option of Naso Alveolar Molding (NAM), a procedure performed by an orthodontist who specializes in treating craniofacial deformities. Beginning in the first few weeks after birth and continuing until the patient is ready for cleft lip repair, NAM gradually brings the palate and lip together and provides symmetry of the nose, preparing the patient for optimal surgical outcomes.
The process uses an appliance consisting of a palatal plate and nasal stent which is made based on an impression of the patient’s mouth. Frequent adjustments gradually tighten the device to slowly mould the palate. Nasoalveolar molding is performed by our specialized orthodontists.
Cleft Lip Repair
3 to 6 months
The goal of cleft lip surgery in Mysuru is to repair the separation of the lip. Cleft lip is typically repaired between 3 and 6 months of age. During those first few months, your child is monitored closely for adequate weight gain and nutrition, and to make sure that there are no issues relative to breathing while eating.
There are a variety of techniques that may be used to repair a cleft lip. The most common type of cleft lip repair is a rotation advancement repair.
The plastic surgeon will make an incision on each side of the cleft from the lip to the nostril. The two sides of the lip are then sutured together, using tissue from the area to rearrange and close the lip as needed. In addition to closing the lip, cleft lip repair realigns the muscle of the upper lip to provide normal lip function and facilitate suckling. In some cases, a second operation is needed. For example, patients with a bilateral cleft lip may require a short hospital stay in order to complete two surgeries, about a month apart.
A primary nasal repair is often performed at the time of lip repair. Although the type of repair differs from surgeon to surgeon, this procedure involves liberating some of the nasal elements and realigning them to a more normal configuration with the use of stents or sutures. Nasoalveolar molding is often used after surgery to maintain this correction.
After surgery for cleft lip:
- Your child may be irritable and feel mild pain.
- Your child may have to wear padded restraints on his elbows to prevent rubbing at the surgery site.
- Swelling, bruising and blood around stitch sites are normal. Stitches dissolve or will be removed in five to seven days.
- Scars will gradually fade but will not completely disappear.
- An intravenous (IV) catheter will be used to give your child fluids until he can drink adequately.
Cleft Palate Repair
9 to 18 months
Goal of cleft palate surgery in mysuru is to fix the roof of the mouth so that your child can eat and talk normally. Cleft palate repair is a more complicated surgery and has the best outcome when the child is slightly older and better able to tolerate the surgery, but before significant speech development occurs. Surgical repair of the palate generally occurs around 1 year of age, following the successful repair of cleft lip if present. In some cases, a second operation is needed.
There are a variety of different techniques that may be used to repair the cleft palate, such as a Z-plasty or a V-Y-pushback. These procedures close the palate in three layers: the inner layers that form the nasal lining; the middle layers, consisting of the muscles at the back of the palate; and the final layer, which includes the oral mucosa.
Palate repair closes these layers while also realigning the palatal muscles, a procedure called an intravelar veloplasty. This puts the muscles in a normal position that allows for the best function of the palate during speech, eating and swallowing.
Surgical repair of cleft palate separates the oral and nasal cavities. This separation involves the formation of a watertight and airtight valve that is necessary for normal speech. The repair also helps with preserving facial growth and proper dental development.
Once the lip and palate are repaired, typically no further surgery is performed for several years. A portion of the palate is usually left open to allow room for the mouth, palate and jaw to grow.
After surgery for cleft palate:
- Your child may experience more discomfort and pain with cleft palate repair than cleft lip repair.
- Your child may have nasal congestion. This can be relieved with medication.
- Your child may stay in the hospital for one to three days and will be given antibiotics to prevent infection.
- Your child will have stitches on his palate. Stitches will dissolve after several days. If packing is placed on the palate, do not remove the packing until instructed.
- There may be bloody drainage from the nose and mouth. It is also normal to have temporary swelling, bruising and blood at the surgery site.
- An intravenous (IV) catheter will be used to help give your child fluids until he can drink adequately.
Palatal Expansion
5 to 7 years (if needed)
Due to the clefting of the alveolus, or gum, and the cleft itself, approximately 25 percent of patients with cleft lip and palate will require palatal expansion as a pre-surgical procedure prior to bone grafting.
The palates in patients with clefts tend to be narrow and collapsed. Palatal expansion prepares your child for subsequent bone grafting by pushing out and aligning the alveolar segments, creating space for permanent teeth. A device is fixed to either the bone or teeth, and with a jack screw, the palate is transversely widened to a normal state. This is done during the mixed dentition phase, when your child's permanent teeth are beginning to develop. The procedure is done by your orthodontist at best hospitals for cleft palate surgery in Mysore, working closely with your plastic surgeon.
Once palatal expansion is complete, alveolar fistulas that were left open at the time of initial lip and palate repair are generally addressed.
Alveolar Bone Graft and Fistula Repair
6 to 9 years
Alveolar bone grafting creates a more complete dental arch, and space for permanent teeth to erupt, by placing bone along the alveolus where it is deficient. Soft bone, generally taken from the hip, is packed in to any remaining opening of the palate. The bone graft is secured with a surgical splint as it heals and solidifies.
At this time, procedures are also performed at best dental clinics in Mysuru to close any fistulas (openings) between the gum and nose. Closing the fistulas with local tissue prevents the escape of fluid into the nose which leads to nasal regurgitation and leakage of fluids during eating.
After the bone graft is placed, permanent teeth may erupt in abnormal positions. Once the bone graft is placed and any fistulas are closed, orthodontic treatment can move teeth into the space created (see Phase I orthodontics).
Phase I Orthodontics
6 to 9 years
Orthodontic treatment may consist of several phases of treatment, lasting several years each. Phase I Orthodontics typically occurs during the mixed dentition phase, when patients begin to lose their baby teeth. In patients with cleft lip and palate, permanent teeth commonly erupt in abnormal positions, so minor orthodontic movement may be required to align teeth.
Planning for orthodontic treatment is generally assessed 6 months after the bone graft is done, and treatment is determined based on each patient’s healing and growth.
Phase II Orthodontics
14 to 18 years
Patients generally begin Phase II of their orthodontic treatment during early adolescence or adolescent years. During Phase II Orthodontics, teeth are levelled and aligned, missing teeth may be replaced, and teeth that are out of position or fail to erupt may be brought down into the dental arch or removed.
This phase of orthodontia includes treatment for atopic eruption of teeth and other potential complications that emerge as a result of bone grafting.
In general, patients with cleft lip and palate may have missing or displaced teeth that have to be removed. Many of these patients, even after final orthodontic treatment and restorations, are missing teeth and may need prolonged orthodontia to move and shape teeth into a more appropriate position. Patients may also need a bridge constructed or dental implants placed. The need for long-term orthodontic treatment varies by the patient.
Orthognathic Surgery (Jaw Surgery)
14 to 18 years
Cleft palate patients commonly have underdevelopment of the maxilla (upper jaw), resulting in maxillary retrusion. In these cases, the upper jaw is situated behind the lower jaw, which is the reverse of the normal jaw placement in which the upper jaw and teeth project further than the lower jaw.
In severe cases of maxillary retrusion, the upper jaw may need to be cut and brought forward in a procedure called a Le Fort I osteotomy and advancement. This surgery is generally done at skeletal maturity, when the patient is between 14 and 18 years old. Follow-up care will include any necessary Orthognathic surgical orthodontics related to jaw discrepancies.
Children seen at a younger age with severe maxillary retrusion may undergo an intermediate phase called a Distraction Osteogenesis. This procedure is reserved for younger patients or adolescents with a severe maxillary retrusion that prevents the jaw from being moved forward in a single stage.
Distraction for severe deformities involves cutting the jaw, applying a halo device called a distractor, and then gradually pulling the jaw forward over a several week period. The jaw is then held in this position for six to eight weeks while the new bone that has been created solidifies.
Cleft Rhinoplasty Surgery
Adolescence or adulthood
As the patient grows, secondary speech procedures and secondary palatal or lip procedures may be done based on the function, appearance and scarring.
Some patients will undergo a final Cleft Rhinoplasty once they have reached skeletal maturity. This procedure may need to be done in stages. Secondary lip revision to improve the scars and correct irregularities may also be performed at this time.
The goal of treatment is to complete all procedures by the time a patient reaches skeletal maturity (usually around age 18). This process sometimes extends well into the late teens or early 20’s due to the complexity of the cases, but the goal is to have the patient finished with their cleft care at this point in time.
Consult the best dentists in Mysore for cleft palate surgery